Hypertension Among Canadian Women: Reducing the Risk.
Being informed can help curb the trend of rising rates of hypertension in women.
By Liza Klassen | March 11, 2021 | Reviewed by Dr. Kelly Clinning ND
Hypertension control in Canada | Hypertension in Women | Reducing Risk | Exercise & Diet and Blood Pressure Health

In 2020, for the first time in decades, the rate of hypertension among Canadians increased1. Hypertension is the leading cause of preventable death and disability in Canada, meaning treatment reduces the risk of adverse outcomes like heart attack and stroke. Unfortunately, rates of treatment and control of hypertension are decreasing, particularly among women over 60 years of age1.
Currently, 1/4 of adults in Canada have hypertension. The rates of hypertension are similar between men and women; however, a smaller percentage of women are taking anti-hypertensive medications. Those taking medication are less well-controlled than their male counterparts1. In a recent survey, only 2/3 of women with hypertension were treated, and less than half had blood pressure levels within a moderate to low risk range. Cardiovascular disease is the single largest killer among women worldwide, with more women than men dying each year2.
Hypertension in Women
Understanding factors that may contribute to the declining rates of hypertension control in women is essential to ensure proper monitoring, management, and prevention. While awareness surrounding hypertension and its long-term consequences is increasing, less than 50% of women surveyed in the United States in 2003 identified heart disease as the leading cause of death in women3. Knowledge is power when it comes to hypertension! Take the time to understand what your numbers mean and what you can do about them.
Increased age is a non-modifiable risk factor for hypertension in both genders. In ageing women, menopause poses an additional risk for cardiovascular disease. Pre-menopausal estrogen levels are protective against atherosclerosis and hypertension, but as estrogen decreases throughout menopause, a woman’s risk increases4. Most cardiovascular events occur in women after 63 years old, partly due to these changes in sex hormones4.
Rates of hypertension are rising, particularly in Canadian women over 60 years old. This cohort of women, between the ages of 45-65, are commonly primary caregivers for both children and ageing parents, known as the “sandwich generation”5. Caregiving impacts an individual’s ability to exercise, eat a healthy and balanced diet and maintain healthy alcohol intake limits5. We know that each of these factors can affect blood pressure levels, suggesting that social factors may be playing a role in the rising blood pressure rates in this group.
Reducing Risk
Gender disparity in hypertension treatment and control is not new. One study found that systolic blood pressure is on average 2.1 mmHg higher in women than in men6. The gender difference appeared at age 55 and above, with a more significant difference seen in women over 601,6. While this difference may not seem huge, every point counts when preventing heart attack and stroke events. Each two mmHg reduction in systolic blood pressure is associated with a 7% reduction in ischaemic heart disease mortality and a 10% reduction in stroke mortality6.
Knowing your numbers or being aware that you have high blood pressure is a critical first step towards efficacious treatment. Regular, accurate blood pressure measurements are vital whether you have elevated blood pressure or not. Understanding what your numbers mean can help you feel empowered to take control of your cardiovascular health.
Making lifestyle changes like adopting the DASH diet*, increasing physical activity, reducing alcohol intake, and stress management techniques can close this gap!
*The DASH diet is especially recommended for people with hypertension (high blood pressure) or prehypertension. The DASH diet eating plan has been proven to lower blood pressure in studies. It is based on an eating plan rich in fruits and vegetables, and low-fat or non-fat dairy, with whole grains. It is a high fiber, low to moderate fat diet, rich in potassium, calcium, and magnesium.
Physical activity provides a positive reduction in sympathetic nervous system activity, helping to keep your arteries flexible, and reducing blood pressure. The type of exercise you choose doesn’t have to be too strenuous; walking, gardening, light jogging, and swimming are all excellent options.
Even losing a small amount of weight can make a significant improvement to your blood pressure, but regular exercise can be of great benefit even if you’re not overweight, so try to make it a lifelong habit.
Here are some of the changes that can make a significant impact on blood pressure levels: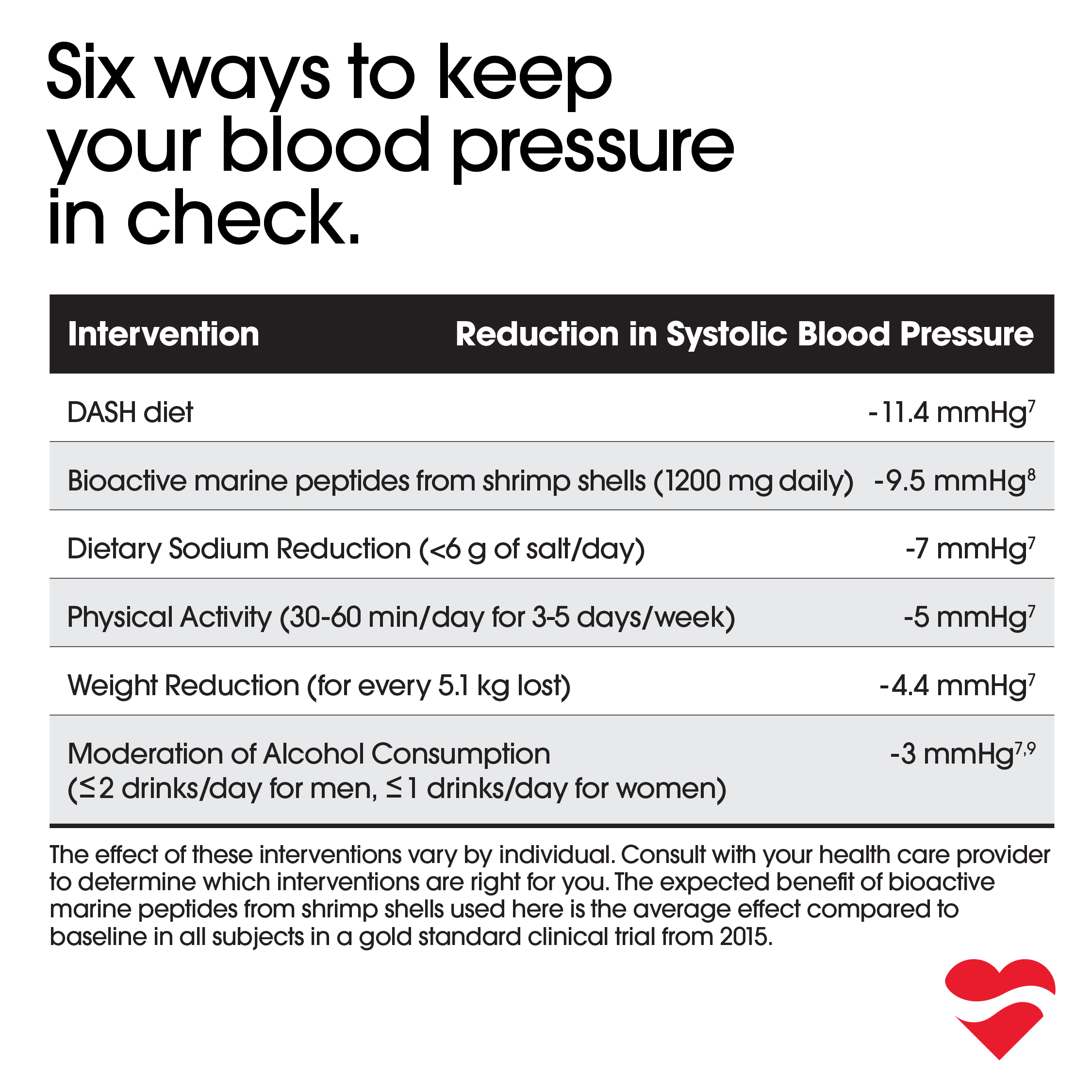
To put these values in perspective a 5mmHg reduction in blood pressure leads to a:
- 14% reduction in heart failure10
- 13% reduction in stroke10
- 7% reduction in ischaemic heart disease10
- 5% reduction in mortality due to cardiovascular disease10
This shows how many opportunities we have to positively impact our heart health and overall wellbeing!
The effect of these interventions varies by individual. Consult with your health care provider to determine which interventions are right for you. The expected benefit of bioactive marine peptides from shrimp shells used here is the average effect compared to baseline in all subjects in a gold standard clinical trial from 2015.
Natural Ingredients to Help Maintain Healthy Blood Pressure
In addition to lifestyle factors, bioactive marine peptides from shrimp shells have positively affected blood pressure in clinical research. In a randomized, double-blind, placebo-controlled clinical trial, bioactive marine peptides from shrimp shells significantly affected blood pressure in eight weeks or less in 89% of study participants. Including bioactive marine peptides from shrimp shells in your blood pressure management plan can contribute to a sense of control, success and, most importantly, help kick start implementing other lifestyle changes like those discussed above!

For more expert advice on blood pressure health, and overall health and wellbeing, visit our growing library of articles at precardix.ca/blog.
Important Information
Always consult with your health care provider before making changes to your blood pressure management plan. PreCardix® does not treat, cure or prevent medical conditions. Measure and monitor blood pressure regularly. Know the signs of heart attack and stroke. Do not take PreCardix® if you are pregnant, breastfeeding, have renal artery stenosis, history of angioneurotic edema or shellfish allergy.
References
- Leung, A., Williams, J., McAlister, F., Campbell, N., Padwal, R., & Tran, K. et al. (2020). Worsening Hypertension Awareness, Treatment, and Control Rates in Canadian Women Between 2007 and 2017. Canadian Journal Of Cardiology, 36(5), 732-739. doi: 10.1016/j.cjca.2020.02.092
- Keyhani, S., Scobie, J., Hebert, P., & McLaughlin, M. (2008). Gender Disparities in Blood Pressure Control and Cardiovascular Care in a National Sample of Ambulatory Care Visits. Hypertension, 51(4), 1149-1155. doi: 10.1161/hypertensionaha.107.107342
- Mosca, L., Ferris, A., Fabunmi, R., & Robertson, R. (2004). Tracking Women’s Awareness of Heart Disease. Circulation, 109(5), 573-579. doi: 10.1161/01.cir.0000115222.69428.c9
- Maas, A., & Franke, H. (2009). Women’s health in menopause with a focus on hypertension. Neth Heart J, 17(2), 68-72. doi: 10.1007/BF03086220
- Parry, M. (2019). Caregiver Burden and Cardiovascular Disease: Can We Afford to Keep the Health of Caregivers in Canada Invisible?. Canadian Journal Of Cardiology, 35(10), 1267-1269. doi: 10.1016/j.cjca.2019.06.025
- Thoenes, M., Neuberger, H., Volpe, M., Khan, B., Kirch, W., & Böhm, M. (2009). Antihypertensive drug therapy and blood pressure control in men and women: an international perspective. Journal Of Human Hypertension, 24(5), 336-344. doi: 10.1038/jhh.2009.76
- Frisoli TM, Schmieder RE, Grodzicki T, Messerli FH. Beyond salt: lifestyle modifications and blood pressure. European Heart Journal. 2011;32(24):3081-3087. doi:10.1093/eurheartj/ehr379
- Musa-Veloso K, Paulionis L, Pelipyagina T, Evans M. A Randomized, Double-Blind, Placebo-Controlled, Multicentre Trial of the Effects of a Shrimp Protein Hydrolysate on Blood Pressure. International Journal of Hypertension. 2019;2019:1-13. doi:10.1155/2019/2345042
- Watson KE, Al Hamarneh YN, Rabi D, Daskalopoulou SS, Tsuyuki RT. Hypertension Canada’s 2020 hypertension guidelines for pharmacists: An update. Can Pharm J. 2021;154(1):19-25. doi:10.1177/1715163520975809
 YouTube
YouTube